
This article leaves me with some questions about the certainty of only posterior dislocations for kiddo. It sounds so incredibly rare to have true posterior shoulder instability with dislocations (as opposed to sublux), but this is what we have been told she has all based off her first dislocation in the 4th grade, which was as a result of being kicked in the back shoulder at school as a child tried jumping over her. I am very curious to know if she has multi directional instability. I am going to read this more closely and do some research and ask the team.
Other questions this brings up:
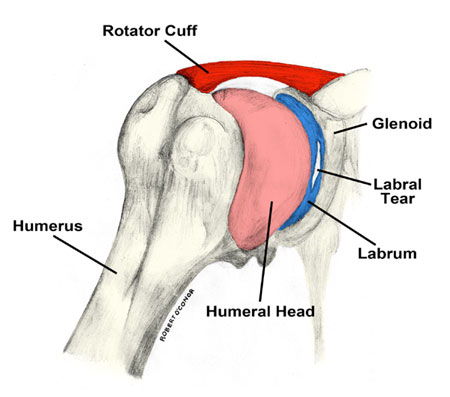
1) How do we know that we have ruled out labral tear worsening or additional labral tears/lesions?

4) Have we ruled out glenoid retroversion/rim erosion?

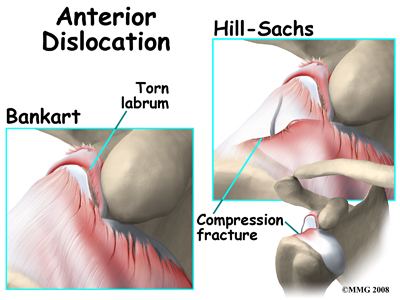
5) Have we ruled out reverse Hills-Sachs lesions?
6) Past MRI reports and doctor reports mentioned thickening of SGHL, but no explanation was given as to if that is important to this ongoing problem. Also, dyskinesis was mentioned in print, but no discussion from doctor as to relevance.
Each of these would need to be known in order to know how to proceed to fix the problem and I don't recall discussing any of these with the orthopedic surgeons with the only exception being that she was said to have a torn labrum that should heal on its own without surgery in 2013. No follow up from that Dr on that issue.
This article (Click here) has good definitions of the types of EDS and says the following regarding hypermobility and surgery: "Shoulder instability in patients with EDS is common.25,29,45 Unlike patients with traumatic instability, patients with hyperlaxity and instability are more likely to experience recurrent subluxation than dislocation.29 The evaluation of shoulder instability has been well described.45 However, because shoulder symptoms in hypermobile patients are not always the result of instability, rotator cuff impingement and other conditions need to be considered.29Nonoperative treatment should be maximized before surgery is indicated.25 When surgery is required, open inferior capsular shift is the gold standard, but the results of arthroscopic procedures may now achieve similar results.29"
I will add articles here, as I find them. If you happen to be reading this, and you have an article to share, please add it in the comments. Thank you.
No comments:
Post a Comment